ABSTRACT
Background: Research has shown the efficacy of hair growth factors in hair regrowth. We describe the intradermal injections of a recombinant, bioengineered hair formulation, containing growth factors, into the scalp skin, for enhancement of hair regrowth and evaluate its efficacy.
Objectives: The objective of this study was to assess the efficacy and safety of the hair growth factor formulation in reducing hair loss and enhancing hair growth.
Materials and methods: This was an open-label, prospective, single-arm interventional pilot study in which 1000 patients were given intradermal injections of a hair formulation into the scalp skin. The formulation contains vascular endothelial growth factor, basic fibroblast growth factor, insulin-like growth factor, keratinocyte growth factor, thymosin β 4, and copper tripeptide-1 suspended in a sterile injectable vehicle. Intradermal injections of this hair formulation were injected into the scalp once every 3 weeks for a total of eight such sessions. Hair pull test was performed before every session. Videomicroscopic and global images were taken at baseline, fourth session, eighth session, and 2 months after the completion of the eight sessions. Relevant safety assessments through
physical examination, questionnaires, and appropriate laboratory examination were conducted throughout the study.
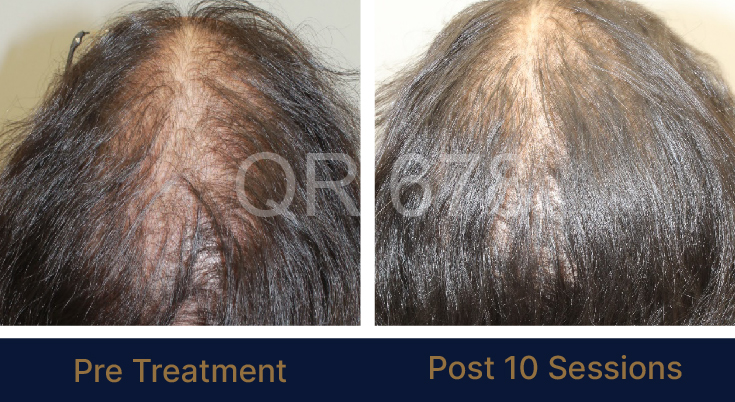
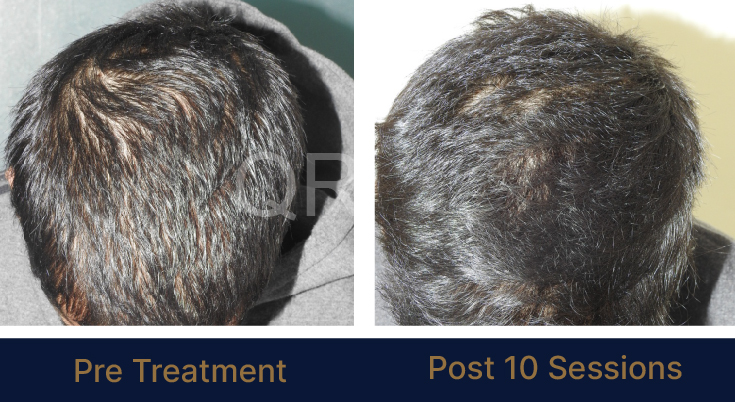
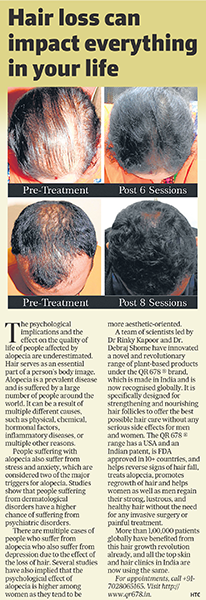
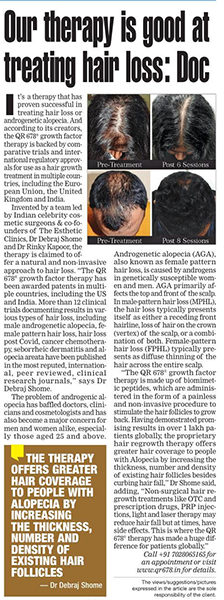
Results: Significant reduction in hair fall was seen in 83% of the patients on hair pull test.
Videomicroscopic image evaluation showed that most patients had a decrease in the number of vellus hairs, increase in number of terminal hairs, and increase in shaft diameter. Seventy-five percent of the patients believed that the hair injections were aiding the treatment of their hair loss, and it was also beneficial in post-hair transplant patients. At 1 year, a statistically significant increase in total hair count ( P = 0.002) continued to be seen. Treatment was well tolerated.
Conclusions: Intradermal injections of this hair formulation may be a promising option for treating male as well as female patterns of hair loss.